
Addie connects hospitals, post-acute providers, and payers in a single AI-powered network — so the right patient reaches the right care, every time.
Hover the cards to explore each part of the Addie platform — or click a care type to jump to the full feature breakdown.
Tailored workflows for iSNP coordination, PACE integration, complex care management groups, and Hospital at Home transitions. Beyond the standard referral.
See every member transition in real time. Guide discharges to your preferred network and automate prior authorization — reduce readmissions.
Receive pre-matched referrals from hospitals that fit your clinical capabilities and insurance contracts. Track referral fit and analytics from one dashboard.
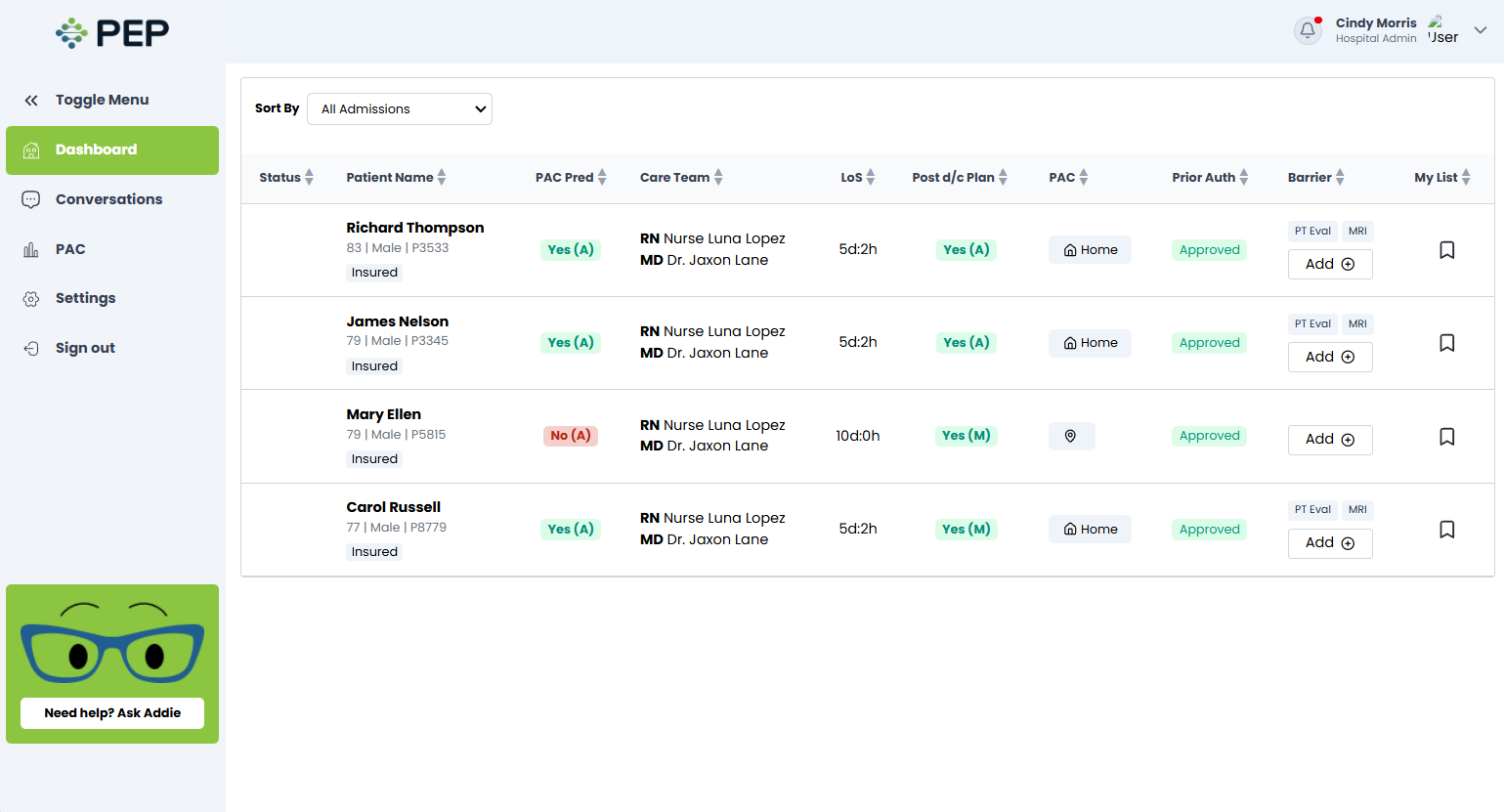
Predict discharge readiness 24–48h early. Match patients to the best PAC partner in seconds. Automate referral workflows inside Epic, Cerner, and MEDITECH — zero extra logins.
Addie gives discharge coordinators real-time AI intelligence inside their existing EHR — so every placement decision is faster, smarter, and safer.
Stop waiting for faxes. Addie sends pre-qualified, clinically matched referrals directly from hospitals — for free, setup in a couple minutes.

Addie gives health plans and MCOs real-time visibility into member transitions — with tools to reduce avoidable readmissions and optimize network utilization.
Addie supports specialized care models that require more than a standard referral — with tailored workflows for each program type.
Institutional Special Needs Plans coordination — connecting facility-based SNP members with the right long-term care placements and ensuring plan visibility throughout the transition.
Program of All-inclusive Care for the Elderly — Addie integrates PACE program referral flows, enabling hospitals to connect members with PACE centers for community-based long-term care.
Complex care management coordination for high-utilizer patients — bridging discharge planning with ongoing community-based care management teams and social determinants support.
Supports hospital-to-home acute care transitions — coordinating home monitoring equipment, nursing visits, and clinical follow-up for patients discharged under Hospital at Home programs.
Addie isn't a tool for one stakeholder — it's the connective tissue between all three. Every new participant strengthens the network for everyone.
AI-ranked PAC matches cut average discharge boarding time — so beds open faster and coordinators focus on patients, not paperwork.
Pre-matched, clinically appropriate referrals mean higher acceptance rates, lower re-hospitalization, and a stronger quality track record.
Visibility into every transition, preferred network steering, and proactive risk alerts drive down avoidable readmissions across the plan.
Start free. Grow with us.
Join the health systems already using Addie to cut boarding time, accelerate discharges, and match patients to the right post-acute care — on Day 1.